
Today, we’ll walk through images from a breast cancer proton plan. From a technical standpoint, Its a unique case for a number of reasons but it does showcase some places and ways in which proton plans greatly outperform what we can accomplish using a traditional linear accelerator with either photons or electrons.
Breast Cancer Treatment: A Study
Some details about the case (mainly if there are other radiation oncologists who see the post). It’s a generalized skin recurrence case – a broad recurrence of chestwall disease. There were a number of positive lymph nodes so the target regions for this case really are just skin and axillary region. I didn’t chase IMC (internal mammary chain) nodes (although they are easy to treat with protons) so they aren’t in the target.
The primary goals of this proton therapy plan were to obtain local control of the rapid skin recurrence and avoid treatment of the lungs and heart. I think this achieves those goals very well.
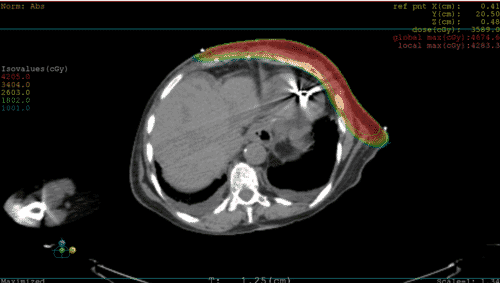
The plan above is single field – it comes in aimed from top right to bottom left – basically aimed right at the heart. With protons, you can do that – you simply stop the beam at the depth you choose.
Prescription level doses are in red – 4205 cGy(RBE). The 1000 cGy(RBE) you can see essentially does not enter the chest. For this particular case, the overall statistics are simply crazy good and not seen for this volume of coverage outside of a Proton Therapy facility.
Comparison of Proton Therapy to Traditional IMRT for Breast Cancer Treatment
The mean heart dose is 0.73 Gy(RBE) – LESS than 1 Gy. The lung volume treated to 5Gy is 3.91%. Basically we are not treating the lung and heart. An x-ray based plan, based on good published data, would deliver about as much radiation to the heart and lungs in this case in 1 fraction as we are delivering in 15 fractions.
Sometimes, a Proton Therapy plan can be just that much better. You couldn’t do this with x-rays – 3D treatment would be along the yellow line. That isn’t viable due to the heart that would be included. IMRT typically gives around 10 – 13 Gy (published data from a really good cancer center) mean dose to the heart – it does shape the high dose region but there is low dose spillage in many areas – IMRT just isn’t that robust in being able to avoid heart, lung and contralateral breast dose. Electrons might cover some but you would have hot spots, match lines, more exit dose and struggle to cover the axilla at midplane in the superior part of the plan (not shown).
If you don’t understand the last paragraph, that is fine. It is there really for more technical aspects. I think the pictures speak volumes. For complex breast cases, Proton Therapy plan often greatly outperform an x-ray based plan especially when considering dose delivered to the heart and lung.
Hopefully this example case allows you to appreciate just how good a proton plan can be at stopping before it reaches the heart and lungs . As always, I encourage you to call a proton facility directly and be an advocate for your own care if you think you might benefit.
Do you know your Gray? (how much radiation your heart receives with radiation) If it is more than 1 Gy, a proton plan will very likely outperform any non-proton therapy plan.
Dr Mark Storey MD