
DISCLAIMER / About the Blog – Please read once if you haven’t. And please note – today, I just talk about traditional fractionation schedules or modestly hypofractionated data.
Today, I’m refreshing a post from may of 2019 where I reviewed prostate cancer radiation outcome data. That post made me focus on intermediate risk disease, and it led me to realize something crazy in the data. This update focuses on intermediate risk prostate cancer.
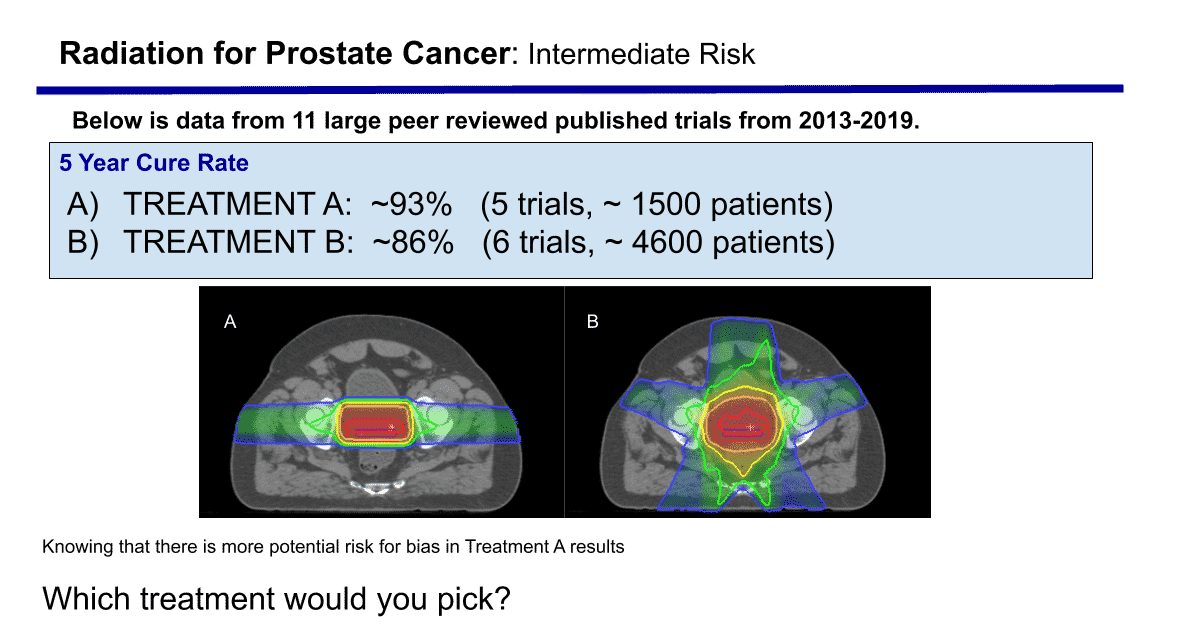
First, I’ll re-post a picture that I built to make people think a bit more about a disease where we often think that good enough is good enough.
Data comparing Proton Therapy to IMRT for Intermediate Risk Prostate Cancer
The above table summarizes the major recent published prostate cancer data. From a research /scientific standpoint, there are inherent significant flaws in using the table without discussing possible issues with this type of comparison between protons and photons.
Problems – all that potentially make Proton Therapy data look better than it is: 1) More data on the photon side is randomized prospective data. In contrast, more data on the proton side is non-randomized data. 2) More data on the photon side is multi-institutional. In contrast, more data on the proton side is single institution data. 3) Follow-up on the photon side is longer than the follow up on the proton side.
These are the three main issues I see with the table. All of these issues lead to significant potential bias in the data and in the outcomes that one can argue make this table irrelevant.
Why I’m not so sure there isn’t a difference and why it may be cavalier to think we know they are “equivalent” when the data looks like it looks.
First off, I think it is important to say that I truly believe the IMRT data is accurate. For intermediate risk disease (which is BY FAR) the most common prostate cancer that I treat, the above table presents well over 4500 patients treated in wide variety of facilities.
IMRT produces results in the mid ’80s for Intermediate Prostate Cancer.
There are 4 reasons I think there is a very real chance that the table actually is correct, representing a real difference, and proton therapy is actually better once you start observing the vast majority of low risk prostate cancer (which I think we largely have done in the US).
1) Nadir data – Everything I’ve seen in my 20+ years of practice leads me to believe that the lower the nadir, the better the outcome. Unfortunately, this data piece STILL doesn’t get published that often. My experience is moving from 7800 cGy to a proton therapy clinic delivering 7920 cGy(RBE) and most weeks I am seeing PSAs for patients that are years out from treatment that I simply did not see with IMRT. 0.2, 0.1, 0.3 etc. etc. I didn’t see these values at near the frequency I’m seeing them in a proton therapy center. I can’t post large tables, but the numbers – in my personal experience – seem to be clearly lower. I tried to find enough to post – and unfortunately haven’t found it yet.
2) PSA Bounce – PSA bounce was first described (from my memory) in brachytherapy for the treatment of prostate cancer. With IMRT, I infrequently saw a PSA bounce. You currently see a PSA pretty consistently in 3 groups of patients treated for prostate cancer – 1) brachytherapy, 2) SRS patients, and 3) Proton therapy patients. To me, somehow – someway – these are going to be proven to be the best option for the treatment of prostate cancer. The important fact is that you do NOT on any significant level see it with IMRT at traditional fractionation. Protons are different – I’ve had to change my clinical practice to educate patients differently – I only did this with implants and it shows up in the Cyberknife data as well. Something with these three treatments is different. Maybe RBE effect at distal end contributes – I don’t have a great answer but something appears different.
3) High Dose Shape – This one is, very honestly, more opinion based – but I have treated prostate cancer to high dose for over 20+ years now. There is a clear difference in the shape of the high dose region between a proton plan and an IMRT plan. Often studies between protons and photons simply look at the high dose and region and say something like – 1/2 the time Proton plans win, 1/2 the time photon plans wins (ie looking at which volume is the lowest cc). Here is a picture of the difference between the two techniques.
There is a fundamental difference in the shape (and I apologize as this gets a bit technical in nature but don’t want to type a book). Due to range uncertainty, we have traditionally overshot laterally in protons even with very high doses of essentially 80 Gy. On the IMRT side, you do NOT get near as wide of coverage. Especially as you dose escalate and or push the dose down on the bladder and rectum. As you push doses down, the high dose region gets narrower and narrower on the IMRT side – just simple physics of the treatment. My argument is that one of the main risk regions is posteriorly and laterally where most of the nerves and blood vessels enter the prostate. I believe the coverage of that region is inherently better with a high dose proton plan than a high dose IMRT plan and I think that is what begins to show up ESPECIALLY once you move beyond the early low risk cancers. It’s actually something I worry a bit about with IMPT. Traditional proton fields essentially “fill” the lower bony pelvis with good dose that extends out nearly to the side wall. To think that this doesn’t accomplish better control in higher risk disease, where we know there are unexpected margin issues from prostatectomy data on a consistent basis, is a bit presumptuous. I think you actually see this in the larger table below – with IMRT you EITHER see low side effects or very good control – not both.
4) The Data Table – If there were ANY IMRT trials in the 90’s I’d feel better. The difference between 92% and 86% is nearly a doubling of the failure rate. Thousands of patients – years of follow-up. Further, we have other supporting reasons that have the data make sense – like nadir, psa bounce, and fundamental differences in the high dose regions. I even included the best number I could find – the Spratt dose escalation data – where patients were treated to the upper 80’s dose wise. It clearly was abandoned due to toxicity, but even there, they could not reach 90%.
For Intermediate Prostate cancer, I think it is very reasonable and appropriate to argue that, based on data, there is very reasonable evidence that their may be a real difference. I think the long term winners in prostate cancer will be SBRT and Proton Therapy (brachy, a great treatment when done in high volume centers, will struggle for different logistical reasons as it has done over the last decade or two). Those are my bets on the long-term victors. Traditional IMRT to standard doses is already falling to the side with modest hypofractionated cases gaining momentum. Whether these can produce results duplicating the best clinical outcomes, to me, is yet to be seen. Below is the original May post.
Note: Above is simply an outcome data argument – I said nothing regarding integral dose, second malignancy etc. which have to favor, to some degree, Proton Therapy.
Summary of Current Prostate Cancer Outcome Data for Patients Treated with Radiation:
Below is a table summarizing recent trials that have been published on prostate cancer. This table simply attempts to summarize current data comparing external beam radiation (both 3D which is older and IMRT which is new since around 2000) to Proton Therapy. It does not include brachytherapy or true SBRT cases.
IMRT is by far the most prevalent form of radiation treatment for prostate cancer and therefore, by default, has been considered the “gold standard” to compare other treatments to – and that is what this table does – it compares Proton Therapy trials to large current (and prior) external beam series.
In total, over 7000 patients are represented. Follow-up is not consistent – newer studies benefit from fewer years of follow-up. These are many of the largest / landmark trials – all published since 2013.
My assessment of the data:
On my look, the photon data (the lower entries in the table) are not as good as the proton data when data is viewed at a very high level. Either you can find trials that have high control rates OR low side effects, but you don’t see both.
A few notes on a couple of series: First: the Spratt (2013) data. It shows excellent control rates and very limited toxicity for grade 3 and higher side effects. The odd part regarding that data is that those patients were treated to 86.4 Gy – much higher than is accepted today. So on some level, those patients must have had more and more trouble as years went by. Otherwise, the standard dose in today’s treatment of prostate cancer would be 85 Gy or higher. I struggle to find the rationale for the move away from that dose in the medical literature. Second: the other notably good result is he Jolnerovski data at 97.5% control for Low Risk disease. It should simply be noted, that trial is 41 patients in the low risk group.
All were treated to 70Gy – 74Gy. Great results. Low risk prostate cancer does very well with radiation in general to doses at current levels. The bladder toxicity is still noted to be high for the entire cohort of 277 patients.
Impact on Intermediate-Risk Patients
If you look at the Intermediate Risk patients, the difference is even more pronounced on the disease free survival side than the difference seen in the low risk patients. For example every recent proton trial published for intermediate grade disease is in the 90%+ disease free survival rate whereas no trials for IMRT have achieved that number (and the two closest to meeting that mark have grade 2 toxicity over 20%). Today, intermediate risk prostate cancer is the largest group of patients that I see. Most doctors these days are doing a good job in active surveillance (watching) the earliest prostate cancers. Most men who present today to my clinic are in the intermediate risk category. We’ve shown (historically) that they need treatment and the goal then becomes the long-term cure of the disease. Control rates in the table above show APPROXIMATELY a failure rate at 2x the failure rate of proton therapy for patients treated with IMRT. That is what the table looks like. The current Widmark non-inferiority trial showed that the hypofractionated arm achieved a mathematical control rate of 78% or better. That is the simplified statement of the math of that non-inferiority trial.
Finally, a statement on high risk patients. To me, this group is the most difficult to assess. The numbers of patients are smaller, the staging and extent of the field size has more variance, the use of ADT and length enters into the equation. The proton data holds up very well and appears superior again. That said, there is good data with pelvic treatment and brachytherapy as an alternative approach so I don’t have as much clarity in this area.
IMRT is deemed to be the “gold standard” due to its prevalence, not because of randomized trial results or because it was first to use high doses.
The history of radiation oncology is that proton therapy has been treating prostate cancer patients to high doses of nearly 80 Gy for ~25 years through the experience at Loma Linda. This pattern – 7920 Gy equivalent in 44 treatments is the most consistent pattern of treatment and has a long and strong track record. On the other side of the radiation technique spectrum, brachytherapy likewise has been delivering very high dose directly to the prostate for 30 years. Many IMRT programs started around the year 2000 and most do treat to doses >75 Gy. It replaced 3D conformal radiation as the standard based simply upon improved radiation plan dosimetry. 78 Gy became the standard largely following release of the MD Anderson randomized trial comparing 70 Gy to 78 Gy showing that higher doses were far more effective at controlling disease (long term data published in 2008 – I helped publish the acute side effect data in 2000 – special thanks to Alan Pollack).
Note: NCCN says they are equivalent treatments. They offer 16 “equivalent” external radiation options currently.
I think that is important to say as well. We do well with treatment for prostate cancer. The above looks at the fractionated radiation data. Like I said, It doesn’t include surgery, brachytherapy, or the various stereotactic approaches that are coming into use. So it is a limited view, there are lots of good options and treatment technique comparisons are difficult. But protons deliver less dose to the patient, they are more targeted, and the data; at least from my view; appears to mirror those facts. I don’t believe there are near as many “equivalent” options, but that is a discussion for a different post.
There is a randomized study available trial comparing IMRT to Proton Therapy.
We’re trying to obtain an answer in a methodical way. Ideally, you don’t use table to compare outcomes, you use studies. There is a large ongoing trial in place. I think over the next 5 – 7 years, it will give more information about what are our better options. It will be slow to accrue but if you are interested in helping to move science forward, it is one I encourage you to ask about.
Related Blog Articles:
Dr. Mark Storey MD
Medical Director, Oklahoma Proton Center