
DISCLAIMER / About the Blog – Please read once if you haven’t.
An extra disclaimer: Some of these post are really pretty easy to write and some of these post are pretty difficult. This one is on the more difficult side as it touches upon a lot of things that people and scientists don’t want to consider. It’s not what is ideal, but rather a discussion on more of what lies behind the scenes within the reality of medicine.
The point of this article is simple – You have to be your own advocate at times in today’s healthcare system. Below I touch upon why for some treatments.
If your doctor does not practice at an institution providing a service (for example, proton therapy) and you are not an advocate for your own healthcare, the odds that you will be referred out of their network is unlikely.
Specifically for Proton Therapy, your care team is very, very unlikely to discuss options for proton therapy when it is out of their network.
On a national level, I think the odds are well less than a single percent it is mentioned to you. In contrast, institutions like MD Anderson or University of Penn or the University of Florida would consider proton therapy in at least 15%-20% (probably 30% but I’ll be conservative) of radiation patients.
Basis for these Statements
Ok – Let’s slow down. So where do these stats or “facts” come from? Good Question.
Honestly, these are just based on my experience. Practicing and seeing referral patterns for 2 decades. But really, to this point, I’ve argued two basic facts –
- “Fact” 1) if you don’t have protons the discussion rate is very very low (I say well less than 1% if your doctors network doesn’t include them).
- “Fact” 2) the more appropriate rate of discussion should be AT LEAST 15% – 20% of patients.
So statistics: We’ll start with the discussion rate for proton therapy and I’ll try to walk you through why it is so low – even though you may have a great radiation oncologist.
“FACT” 1: THE DISCUSSION RATE WILL BE MUCH LOWER THAN IF YOU ARE AN ADVOCATE AND ACTIVELY QUESTION YOUR OPTIONS.
At anytime during this post, do NOT think that I am saying, “if I potentially benefit and my doctor doesn’t discuss proton therapy, they are bad”. That isn’t the case at all. I know because I now believe I dramatically under-referred for proton therapy for decades. I don’t think I was bad, but I could have been better but there are real obstacles from an MD side that make sending patients for proton therapy incredibly difficult.
So I’ve made an abrupt transition professionally. I’ve moved from a state with no proton therapy to a center where, largely, we only have proton therapy. Realistically, it is as big of a move as one can make – and it gives perspective. Here are the main issues that I see.
1) THE VAST MAJORITY (PROBABLY >90% OF RADIATION ONCOLOGISTS) HAVE NEVER SEEN, IN ANY HANDS ON WAY – A PROTON THERAPY PLAN.
In and of itself, that is a huge hurdle. So an example: I’m in Arkansas and I haven’t been to a dedicated proton meeting (because outside of those meetings, there frankly isn’t a lot of time spent on protons – in fact, I recall that at every ASTRO meeting I’ve personally attended, if anything, it is a negative to be in the proton space and often gets some laughter or chuckles when mentioned). So you are practicing and you don’t have a proton machine and there is not one on the horizon for your institution – because as an MD you really can’t go solo on a 50+Million dollar project. A patient comes in, and maybe you’ve done really good and read or have someone you know who has experience, and you think maybe protons might help. Realistically, you don’t know if you haven’t planned proton cases. Your planning system has NO ability to show you a comparison plan. If you have a friend who is an MD, you can call them and get an idea. Logistically, you have a cancer patient coming to see you and your option is either to address what you know or to add in the variable of – maybe, if you travel out of state to somewhere like MD Anderson, after they do an extra couple of weeks of workup – there might be a better radiation option – maybe, but maybe not. Throwing that into the conversation of caring for a cancer patient is NOT easy. In your first interaction, you have talked about a huge area where you realistically can’t give real answers and worse – many patients are NOT good proton patients or struggle with insurance coverage. If you don’t know who to send, how can you send anyone? So very often they don’t.
Until a far larger percentage of radiation oncologists have used proton therapy, we’re going to struggle.
2) ADMINISTRATIONS DON’T LIKE TO SEE PATIENTS SENT OUT OF “THEIR” SYSTEM.
An occasional or really rare case – fine. Maybe a small subset of some cancer – ok. A steady stream of patients leaving the system isn’t consistent with the advertising and overall business model. It’s as simple as that.
3) AS A RADIATION ONCOLOGIST, YOUR PARTNERING PHYSICIANS IN YOUR PRACTICE AND IN OTHER SPECIALTIES WOULDN’T LIKE IT.
It complicates the entire care of the patient to send someone out of network. It’s hard to get records. It brings up questions like, why didn’t my prior doctor tell me about them? Physicians, like it or not, are often paid by volume of work. Referring out of the system on any consistent level makes your administration and other in network treating physicians not as pleased as simply not rocking the boat and keeping everything in house.
4) NO GOOD KNOWLEDGE OF THE INSURANCE ISSUES.
Unless you live in the proton therapy world, there is literally no way that you can understand which cases are covered and which are not. Which insurance plans cover what disease sites and which indications and which ones do not. It is state by state, contract by contract information that you cannot find. You are sending someone, often many miles away only to have them potentially be denied by their insurance. If you think that doesn’t feed back into items 2) and 3) above…well, it does.
5) SOME PEOPLE DON’T THINK IT IS BETTER.
They argue for more trials and studies. Longer follow-up etc. Mainly these are often cost arguments hidden in a veil of clinical discussions but there are some who do feel strongly that more data is required before they send a single patient. If the cost was the same and they were blinded to the plans, they’d pick protons probably 70% the time. (my opinion).
Learning About Proton Therapy
I understand the ideal for physicians: spend time – learn protons – educate your patients – be idealistic in your practice.
So how do you learn protons? The simplest way would be: go to a couple meetings. That would begin to give you an idea. Let’s say it starts to address – item 1) above. It’s not hands on, but it’s better than nothing. You now might think it’s better but still have significant barriers and not understand when and how insurance will affect your patient’s care.
Aside from that option, you need some luck and probably a couple of years to transition your career. I got lucky and it took me about ~2 years to transition my career. What were my other options if this job in OKC didn’t come together – let’s see, I looked at Proton Fellowships – essentially going back to school to make a small fraction of what I was making – that was an option. Taking about 3 months off from practice to simply go to MD Anderson to shadow staff – since I trained there, I could have likely done this – I couldn’t help or practice without a Texas license – that takes a few months to get but I could have. It would have been a non-paid vacation. It would have hurt my practice. It would have hurt my partners, but because I was fortunate to train there, I probably had it as an option.
Honestly, I’m not sure that there was any other path shorter than a 5-10 year plan to get something built in Arkansas. There are NO good options to train practicing busy radiation oncologists on new modalities that are not available in their practice.
The typical path of “go to a meeting and talk your administration into purchasing” doesn’t really work at the $50+M price tag.
The hardest part about all of these options is actually – in simple terms – you are doing it with the idea that you are going to learn about something that isn’t available and if you begin to use in your practice, will hurt your career where you live currently. That’s a big ask. Not many will do take on that task.
So there are good reasons why you can be a good radiation oncologist and not really understand or utilize the benefits of proton therapy. – these issues lead to an significant under-referral rate to outside proton centers in my opinion.
At the end of the day, I think the long-distance (>60 miles) discussion rate for proton therapy is a fraction of a single percent. So my guess is like 0.3% of patient will be discussed the option of proton therapy for Head and Neck cancer, or concurrent treatment for Lung, or Esophageal cancer – that is my estimate on a conversation / discussion rate – the actual referral rate is less than that. It is based on data – I helped lead care for 10000+ patients in a 5 year span. I’ve joined other people from other communities here in OKC and we all place the discussion rate in a low fraction of a percent if it is out of network.
There are small pockets or practices that are very close to a proton therapy center where it is discussed more frequently but mathematically they are small. But it still is discussed as an option WAY TOO INFREQUENTLY. Here – in Oklahoma City my guess for the community is that it is brought up by the MD about 5%-10% of the cases that potentially benefit – so not a 20% discussion rate – a 1%-2% discussion rate – 5% to 10% of good proton eligible candidates. This is in a local community with 10 years of history of proton therapy. Even here, there still are significant hurdles to having any routine pattern of referral outside of your network. It just doesn’t happen that often.
FACT 2: THIS ONE IS EASIER – CLEARLY IT SHOULD BE DISCUSSED AT SOME VERY SIGNIFICANT RATE IF YOU BELIEVE THAT PATIENTS WOULD LIKE TO BE EDUCATED ON OPTIONS – SO BASICALLY JUST 4 PICTURES.
So what are some patients that get us to a discussion rate of 15%-20%.
HEAD AND NECK CANCER: BASED ON THIS SLIDE, I’D SAY HAVING A DISCUSSION IS REASONABLE EVERY TIME.
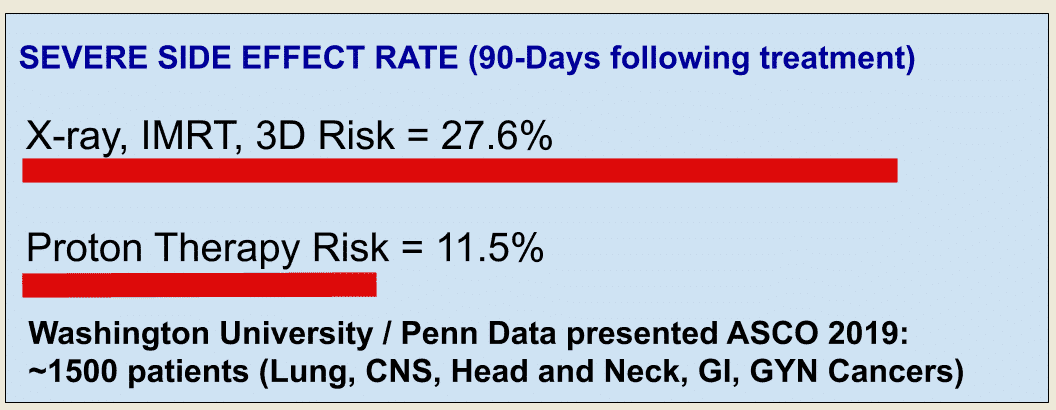
LUNG, BRAIN, GASTROINTESTINAL AND GYNECOLOGIC CANCERS TREATED WITH CONCURRENT TREATMENT.
AND ALL PEDIATRIC PATIENTS REQUIRING RADIATION.
So in summary, the discussion rates are very very low. If you want to know if you are a good potential candidate, you often have to be an advocate for your own care and inquire.
Dr. Mark Storey MD