
DISCLAIMER / About the Blog – Please read once if you haven’t.
Today we’ll look at total integral dose delivered to the patient across a variety of cancers treated with radiation.
Here is the crazy part of this post:
For most treatments, much more radiation dose is delivered in normal healthy tissues than the target.
This is and has basically been the case for the vast majority of external beam photon radiation treatments. It continues to be the case with new treatment approaches like IMRT (intensity modulated radiation treatment) or SBRT (stereotactic body radiation therapy) or SRS (stereotactic radiosurgery) or Gammaknife or anything using external photon delivery. In fact, as the target gets smaller, the relative amount deposited in the tumor often gets to be a very low percentage of the total radiation dose.
Protons have better treatment properties. They deliver lower dose before the cancer and stop in the target. This results in proton plans typically reducing dose to normal tissues by 30%-60% over external beam photon radiation plans. They aren’t a perfect answer by far. But they are often able to get about half the dose delivered into the target. This is a large scale improvement over traditional external beam radiation in many areas.
This is really a little talked about fact that most people, even radiation oncologists, probably don’t realize just how much of the treatment ends up in normal tissue. But it is real and it is the physics and math of treatment.
Does that matter and is it “worth” it?
The body is an amazing structure and it heals and recovers amazingly well from damage. Think of breaks or cuts or even surgery. Often times, you heal really very well. Generally there are some effects from any major injury but the body heals and the mind also learns simply how to deal with the issue. We are great adaptive creatures and that is truly a blessing. So, from a physician perspective, for many years protons were NOT available. You had no option, so you learned and trained with photons. You did the best you could and often you relied on the bodies great ability to heal from lesser degrees of damage and heal remarkably well in many instances. Over time, you think it doesn’t matter or matters soooo little that it isn’t worth the trouble.
I think about it differently. I’m an engineer and math / science person at heart and I very strongly think that we’ll use the better treatment properties of proton therapy to continue to improve outcomes for an ever increasing percentage of the population over the next decade. Less radiation is better and we’ll show it. Even with the history of Proton Therapy now several decades old, we are just on the cusp of its development and integration into cancer care on a broad level.
The Role of Radiation Oncologists
The job of the radiation oncologists – every day, in every clinic – is largely to develop the “best” plan that treats the least normal tissues. If they were blinded to delivery and costs, I strongly believe it would be utilized for at least 20% of cases today.
Really I think the number today is 25% – 35% but I’ll put a conservative number in bold 🙂 We pick the “best” plan because we know that radiation isn’t good and that limiting dose to the target and limiting dose to normal tissues is the goal. Proton therapy is no different. It simply isn’t available and it has been very expensive to produce over the last decade so this leads to the argument of is proton therapy “worth” the cost. So we’ll look at some sites today and run through what plans look like between IMRT and proton therapy plans.
So a proton plan is 30%-60% better? No.
Don’t confuse integral (total body absorbed dose) to the plan result. It is ONE component of the plan. The strength of the plan is assessed by several factors. From around 2000-2015, we didn’t look at total absorbed dose that much. We made strides with computer technology focusing the high dose regions better to the target while increasing the total dose delivered. So below, I’m mainly looking at the total integral dose aspect of the plans and the difference in this particular aspect of the plan evaluation.
HEAD AND NECK CANCER – PROTON THERAPY VS. IMRT
So the first case is a head and neck case – specifically a nasopharynx case treated with IMPT – fancy current cutting edge technology used for complex cases. This is actually one where a lot of the radiation for the photon plan (external beam IMRT plan) hits the target. I picked this example because this is actually one of the case where the difference is the LEAST between the two modalities with respect to the question of where the dose gets deposited. Even here where the IMRT does a good job, there is really no comparison. The volume of unnecessary radiation is shown on the right and those colors represent real short and long-term side effects. My educated guess is that this IMRT plan probably delivers about 50% of the dose or more within targets that your doctor wants to treat. This is an example of a case where Proton Therapy is critical and why we have to push for better availability of this technology.
PROSTATE CANCER – PROTON THERAPY VS. IMRT
Next we’ll look at a prostate cancer case treated with uniform scanning protons. In this case, Proton Therapy really wins and wins very easily with respect to total dose absorbed by the patient. I’ll ballpark the numbers – for IMRT or SBRT or whatever “fancy” technique is used with external beam radiation, about 3/4th’s of the radiation dose lands OUTSIDE of the region at risk for cancer. For a Proton Therapy plan, about 1/2 of the radiation lands INSIDE the region at risk for cancer. These numbers bounce around a little so there isn’t a hard / fast rule other than to say – a lot more radiation ends up in the patient with IMRT than with Proton Therapy.
Some will argue this doesn’t matter. I believe less radiation will be proven to be better in the long term. I think the data today supports better outcomes and less side effects when viewed objectively. I also believe the long term data will show a larger separation due to the increased risk of second malignancy due to the extra radiation in the IMRT plan. This will take 10-20 years to appear in data but there are studies of the SEER data that this difference is beginning to be verified in clinical outcome data.
BREAST CANCER – PROTON THERAPY VS. EXTERNAL BEAM – A MORE COMPLICATED ANSWER.
Now we’ll look at a case where the total absorbed dose is probably pretty similar between the two techniques. I don’t want anyone to think that I believe Proton Therapy is a fix all or required for all cases. I do believe there are a good 25% to 40% of cases where Proton Therapy will be the standard the care over the next decade, but that isn’t all cases. So let’s discuss a case where Proton Therapy doesn’t help and the dose for external beam photon treatment all goes basically where you want it to go.
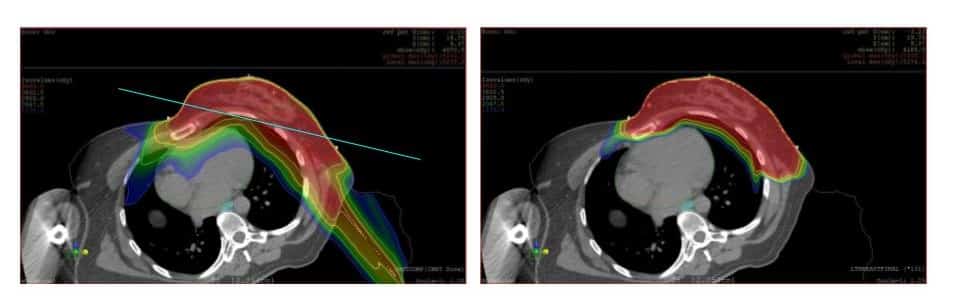
Many early breast cancer cases are a great simple example where 3D external beam does a great job for straightforward early cases. Cases where the tumor is away from the chest and the heart and simple tangent radiation fields can treat the breast, traditional treatment with simple tangent fields is the best options. This represents the majority of breast cancer cases.
So in the image below on the left, I’ve drawn a bright blue line. If your doctor only needs to treat “above” that line for a early breast cancer then likely around 90% to even 95% of dose from a 3D radiation plan will go to the intended target using external beam photon therapy. A Proton plan might change that a very small amount but in simple terms, it would not help and would make the treatment more complicated. That patient is best served today with 3D treatment (not IMRT) – 3D treatment with tangent fields is simple, proven, straightforward and is often the best radiation option.
That said, there are many instances where Proton Therapy may significantly reduce dose to the heart or other structures and should be evaluated:
- If they are using IMRT for your breast cancer (hint: they are trying to miss something)
- Left sided breast cancer
- If they need to cover lymph nodes because the cancer went to the nodes
- If the cancer is very far medially (towards the center) on the breast
- If a mastectomy was required
These are cases where it is very reasonable and appropriate to look at Proton Therapy. Even though the majority of the dose will go to the target, the improvements in the Proton Therapy plan are worth evaluating.
In the case shown above, the patient has an advanced breast cancer. Lymph node treatment is required. Here Proton Therapy dramatically reduces dose to the heart. This is a typical result when comparing photon treatment to Proton Therapy. The “typical” result cuts the long term risk of coronary disease by half based on recent data from one of the two largest cancer hospitals in the nation (I’ll leave the name out) but the two papers, one from 2019 and one from 2018, when compared, show that proton therapy is far better option for locally advanced cases reducing dose to the heart by a factor of 10 with the use of Proton Therapy.
Simply stated – there is great room for improvement with advances in technology in the field of radiation oncology. Radiation is a critical component of cancer treatment and improves survival for many patients diagnosed with cancer. It is an exciting time to be in this field of medicine.
SUMMARY: PROTON 101 – WHERE DOSE GOES
With external beam treatments (including IMRT, SBRT, SRS, Cyberknife, Gammaknife), for most plans, most of the dose misses the target, so there is lots of room for more targeted approaches.
I believe strongly that integral dose in radiation therapy is important. In the relatively short history of radiation oncology, it was a primary driver of plan assessment for about 30 years. For about 15 years, during the development of IMRT, we moved away from emphasizing it. More and more it is returning. You see that through Proton Therapy center development or the addition of very low dose constraints that have emerged in the last decade as we realized that low doses matter. I believe integral dose evaluation is returning to the clinic as one of the central metrics we will use to push side effect risk down over the following few decades. Particle therapy will be a centerpiece of that shift.
Dr. Mark Storey MD
Medical Director, Oklahoma Proton Center